|
 |
|
 |
 |
About Us | Contact |
|
|
01/06/2011 - CRUK lets public down over mobile phone advicePowerwatch condemns Cancer Research UK over lack of mobile phone safety advice. Cancer Research UK (CRUK) has long played down the possibility of any association between mobile phone use and cancer. OK, so that has been their interpretation of the data as they see it. Now the World Health Organisation's International Agency for Research on Cancer (IARC) has had 31 of the world's best experts in these matters looking at all the evidence. They have concluded, almost unanimously, that there is enough evidence to classify Radio Frequency energy exposure as a "Possible Human Carcinogen" (IARC Class 2B). The evidence is mainly from human studies but also from animal and cell studies including some feasible mechanisms of action. Much of the evidence they based their assessment on is from mobile phone studies. You would think that CRUK would now accept the IARC judgement and promote more cautious use of mobile phones, especially by children and young people.
Instead, they virtually dismiss it as being most unlikely and do not offer any advice to the public or users about ways they might use their mobile more safely. We do wonder which team they are playing for. Ed Yong, head of health information at Cancer Research UK, said: "The vast majority of existing studies have not found a link between phones and cancer, and if such a link exists, it is unlikely to be a large one. The risk of brain cancer is similar in people who use mobile phones compared to those who don't, and rates of this cancer have not gone up in recent years despite a dramatic rise in phone use during the 1980s." We believe those statements to be exceptionally misleading.
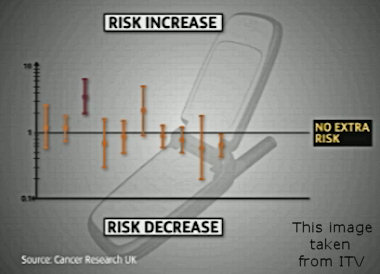
On their website they report the IARC decision. Then they display two graphs purporting to show the state of research on these matters. Both graphs are what we would expect from the wireless industry but not from a Charity interested in helping the public. Solid tumours usually take a minimum of 5 and typically 10 to 25 years to be diagnosed from the time they start to grow. CRUK know this. Most of the studies they show had virtually no people with that length of mobile phone use. So to lump all the studies together as CRUK have done and "average them out" is, in our opinion, not worthy of a school project and not what we deserve to see from a leading cancer Charity who should, and do, know better. The meta-analyses of the studies for people who have used a mobile for more than ten years show significantly higher incidence rates (variable but around twice as many i.e. a doubling in likelihood of developing a glioma — which are often then fatal within a few years of diagnosis) among long-term phone users when compared with non-users or short-term users. CRUK fail to mention that all the positive data associating brain tumours and parotid (salivary) gland tumours with mobile phone use is in people who have used a mobile phone for more than ten years. They are also misleading people about UK incidence of brain tumours over time. Whilst overall numbers are remaining fairly stable, there is a strongly statistically increased incidence in malignant tumours in the temporal and frontal lobes diagnosed in England over recent years. These are usually gliomas and are typically fatal within 3 to 5 years of diagnosis even with extensive and painful treatment. See below for more details (mostly extracted from an earlier news story of ours). Unlike Ed Yong of CRUK, Dr Christopher Wild, Director of the IARC, said: "Given the potential consequences for public health of this classification and findings it is important that additional research be conducted into the long term, heavy use of mobile phones. Pending the availability of such information, it is important to take pragmatic measures to reduce exposure such as hands free devices or texting." Now that is excellent and appropriate advice. WHO estimate that there are five billion mobile phone subscriptions globally, so even a small increase, let along a doubling, could result in large numbers of extra brain tumour cases. A doubling in incidence would result in something in the order of an extra 250,000 brain tumours per year every year in people with more than ten years mobile phone use. That would be a very serious world public health problem. It seems to us that Cancer Research UK are still more interested in developing treatments for cancer rather than preventing it in the first place. This criticism has been made about them several times over the years. Currently they spend most of their money on surgical techniques and new drug treatments for existing cases. They spend a tiny percentage of their income on researching real "prevention". Surely prevention is better than cure? If you are considering donating money to CRUK or planning to leave them a legacy in your will, then you might like to also consider specifying that the money must be used for work on cancer prevention, including issuing appropriate precautionary advice to the public.
Three meta-analyses of case-control studies have concluded that that using a cell phone for more than 10 years was associated with an increase in the overall risk of developing a brain tumour.[Refs 1,2,3] All three found statistically significant more brain tumours in people who had used a cell phone for more than ten years and one study reported a doubling of glioma on the same ("ipsilateral") side the cell phone was used (118 cases, OR=1.9; 95% CI, 1.4-2.4). Although the Interphone initially reported an overall reduction in risk associated with mobile phone use, more refined analysis by the authors later showed a doubling in glioma incidence for over ten years regular mobile phone use (190 cases, glioma OR=2.18, 95% CI, 1.43-3.31) with a similar result for cumulative hours call time. [Refs. 4,5]
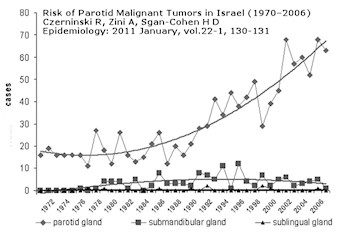
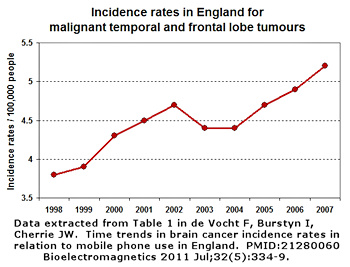
Earlier this year Rakefet Czerninski and colleagues published a paper looking at parotid gland cancers in Israel over the period 1970 to 2006 [7]. Whilst other salivary gland tumours remained stable at low levels, the incidence of parotid gland tumours (in the side of the head close to where a mobile phone is held) rose four-fold. This is shown in the graph on the left. There may be another explanation though no-one seems to be able to offer a reasonable one. If it were better diagnosis, the other salivary gland tumours would also be on the increase. No overall rise in malignant brain tumours is yet showing in most national cancer statistics, though de Vocht has recently reported what we interpret as a worrying recent rise in UK Office for National Statistics cancer registry data for England [6]. The change in incidence of temporal and frontal lobe tumours (close to where most radiation enters the user's head) is shown in the graph on the right that we have derived from their published data. The slight fall in 2003-2004 can be also seen across various non-brain cancers in ONS data and is likely to be a cancer registry recording artefact. There are plenty of good, peer-reviewed, scientific reports in the literature showing evidence of biological effects that are likely to lead to adverse effects on health and well-being. We have prepared a list of 150 selected studies as a XLS spreadsheet, also as a web page, with main authors, title, journal and PubMed hyperlinks so that you can easily go and see the details. These are all concerned with exposure to mobile phone signals at specific absorption rates (SARs) below the 2 W/kg level that is set as the maximum allowed from a mobile phone handset in Europe. Yet in 2009 the EC's SCENIHR working group still concluded that there was no need for any precautionary action such as specific advice for children's use of mobile phones, though they did call for more research. Another forthcoming Interphone study confirms an increase in acoustic neuromas, a less dangerous cancer of the acoustic nerve, on the side of the head where the mobile is most frequently used. References
This page has links to content that requires a .pdf reader such as |