 |
 |
|
 |
 |
About Us | Contact |
|
|
Poor Interphone Study Design Underestimates Brain Tumor RiskInterphone Studies to Date, An Examination of Poor Study Design,
|


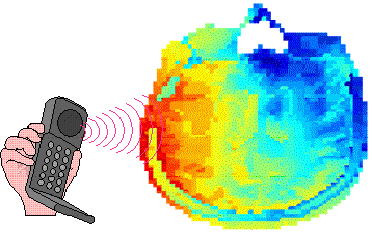 Figure 2, Exposure of the Brain Taken from ISEE/ISEA Congress, Paris - 5 September 2006 |
The colors in Figure 2 indicate the Specific Absorption Rate (SAR) of cellphone radiation. SAR is the amount of power absorbed by tissue, in this discussion, brain tissue, in Watts per kilogram. The colors show the SAR distribution in decibels, a logarithmic scale (red is highest, orange is much smaller, green is very low, and blue is no exposure.
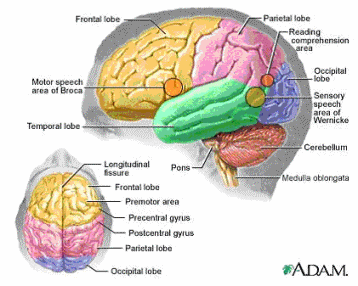
As seen in Figure 1, for brain tumors, the temporal lobe (green) and the acoustic nerve, the nerve from the ear to the brain (not shown), absorb almost all of the cellphone's radiation plume. Certainly, as seen in Figure 2, the plume is only a small portion of the brain and is entirely on the side of the head where the cellphone is used. In Figure 3, we see that the depth of the cellphone's radiation plume's penetration is quite shallow. More that 67% of the radiation plume's power is absorbed within an inch (2.54 cm) of the surface of the skull.
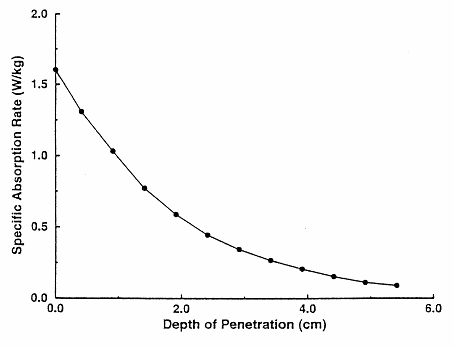
Figure 3, Depth of Cellphone's Radiation Plume
Taken from ISEE/ISEA Congress, Paris - 5 September 2006
Studies that include brain tumors outside of the cellphone radiation plume underestimate the risk of brain tumors.
Flaw 3: Latency Time and Definition of Regular User
The third flaw is the definition of "regular" cellphone use in relation to a reasonable latency time. "Regular" cellphone use is defined as use of a cellphone on average once per week for at least 6 months. Exposure within 1 year of the diagnosis date is not considered. The result of this definition, combined with the incredibly fast rate of new cellphone users, is to overweight "regular" users with an incredibly large group of short-term users?far too short a time to expect a tumor to be diagnosed.
Let me illustrate using USA cellphone subscriber data by year. US data is available, while for most other countries it is not available. It is used here to illustrate how the inclusion of "regular" cellphone users results in highly distorted findings and not to indicate that countries where the Interphone studies occurred.
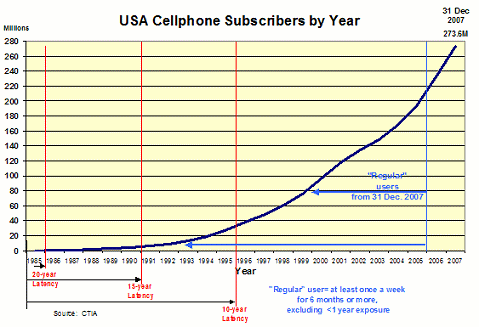
Figure 4, US Cellphone Users by Year
Latency time is the time from an exposure to the diagnosis of a tumor. What we know about the latency time for brain tumors comes from ionizing radiation exposures.4 Based on ionizing radiation, the latency time for brain tumors is between 25 and 40 years, similar to the latency time of lung cancer from tobacco exposure. Figure 3 shows 10, 15 and 20 year latency time in relation to the number of subscribers. Intuitively we can see these latency times are a very small proportion of "regular" cellphone users.
For the 9 Interphone studies, using weighted averages for cases or controls, we see that 0.61% of cases and 10% of controls have used a cellphone for 10 years or more, and 18% of cases and 21% of controls have used a cellphone for 5 years or more.
The result: for a reasonable latency time, it would be unlikely to find any risk of tumors, given the percentage of cases and controls. Yet, as we saw in the Studies on the Risk of Brain Tumors from Cellphone Use section, there is a risk. "It would appear that when a cellphone is used for > 10 years and the tumor is on the same side of the head where the cellphone is used, there is a significant risk of a brain tumor."
Because such a large percentage of "regular" users have used a cellphone for an unreasonably short latency time the reported results for < 10 years5 as well as for > 10 years (6.3% of cases) are an underestimation of risk.
Flaw 4: Children and Young Adult Are Not Included in Interphone Studies
The Interphone Protocol states that cases be between 30 and 59 years of age While a few studies have included cases as young as 20, the non-inclusion of < 20 year olds results in an underestimation of risk. Why? Because children, with their high rate of cell division, are at higher risk of tumors than adults. As we know there a considerable proportion of cellphone use by children. And, we know that children, especially teenagers, spend more time on cellphones that do adults.
Flaw 5: Cellphone's Radiated Power
It is reasonable to expect that risk of a tumor from a cellphone, after a reasonable latency time, would be the cellphone's power multiplied by cumulative time of use. In the early days of cellphone use all cellphones used analog technology. These always radiated a fixed amount of power (~2 Watts). Analog cellphones use has been totally displaced by digital cellphones. Digital cellphones have a feature called Automatic Power Control or APC. At the beginning of a call the cellphone radiates maximum power (~2 Watts) but quickly reduces the power so the radiated power is sufficient to have a reliable link to the cell tower (AKA masks or base stations). The result is that cellphones radiate far less power in urban areas compared to rural areas. This is because cell phone towers are much closer in urban areas compared to rural areas so the cellphone radiates less power in urban areas and more power in rural areas. When rural and urban cellphones are not reported separately the result is an underestimation of risk.
Flaw 6: Number of Cases Included in a Study
The weighted average time in these 9 studies for a case to be eligible for inclusion in the study was only 2.6 years When one considers 4 of the 5 previous flaws, it becomes obvious that such a short period of time for eligibility will result in too few cases to resolve these flaws. For example, if tumors were limited only to the exposed region of the brain then there would be far fewer cases; if a reasonably long latency time was included, again there would be far fewer cases;6 if children had been included there would have been more cases; and, if rural users were to be compared to the far larger number of urban users a much larger number of cases would need to be eligible to participate in the Interphone Study.
4 - Cellphone radiation is non-ionizing radiation.
5 - ypically < 10 years is actually 5 to < 10 years.
6 - When there are too few cases the statistical power to determine if there is a risk is lost. A rule of thumb is that 30 cases are required to give any chance of a meaningful result.
Conclusion and Discussion
With five flaws, each independently underestimating the risk of tumors, it is no wonder why the Interphone studies report a large number of results suggesting cellphone use protects the user from having a brain tumor.
The Interphone Study has substantial funding from the cellphone industry. The additional cost to resolve these flaws could have been accomplished if the industry provided more money. In addition if the participating countries had anticipated the potential cost of a pandemic of brain tumors, the cost effectiveness of contributing substantially more funds, would have been obvious. Lastly, relying on the cellphone industry funding is equivalent to having the fox guard the hen house.
The cellphone industry will state that there is a "firewall" between their funds and the research teams who do the studies. While it is true that the cellphone industry provides the funds to another organization (UICC)7 which then decides on the teams that will do each study, the researchers are aware that most of their funds are coming from the cellphone industry. While I do not doubt the integrity of the researchers, I also believe there in an inherent conflict-of-interest, best described by the saying, "Don't bite the hand that feeds you."
7 - UICC | international union against cancer
The fundamental problem is not conflict-of-interest. The fundamental problem is the Interphone Protocol. While I have no evidence, it would appear that the cellphone industry influenced the Protocol, if not actively participating in its creation. The end result is the Protocol is designed to not find any risk. That it has found a risk is sobering.
Tragically, the window of time to do a large, well-designed case-control study is closed. Case-control studies require exposed and unexposed subjects. It is no longer possible to find unexposed subjects.
References
[1] Schoemaker et al, (October 2005)
Mobile phone use and risk of acoustic neuroma: results of the Interphone case-control study in five North European countries, British Journal of Cancer. 2005 Oct 3; 93 (7): 842-8.
A Scandinavian and United Kingdom Interphone Study reporting, "The risk of acoustic neuroma in relation to regular mobile phone use in the pooled data set was not raised ..."
[2] Lahkola et al, (2006) Mobile phone use and risk of glioma in 5 North European countries, International Journal of Cancer: 120, 000-000 (2006)
A Scandinavian and UK Interphone Study reporting, "We found no evidence of increased risk of glioma related to regular mobile phone use ..."
[3] Lonn et al, (2004) Mobile Phone Use and the Risk of Acoustic Neuroma, American Journal of Epidemiology 2004; 159:277-283.
A Swedish Interphone Study reports, "The overall odds ratio for acoustic neuroma associated with regular mobile phone use was 1.0." [i.e., no risk]
[4] Christensen et al, (2004) Cellular Telephone Use and Risk of Acoustic Neuroma, American Journal of Epidemiology, Vol. 159, No. 3, 2004;159: 277-283.
A Danish Interphone Study reporting, "We did not observe increased risk of acoustic neuroma among regular cell phone users ..."
[5] Lonn et al, (2005) Long-Term Mobile Phone Use and Brain Tumor Risk, American Journal of Epidemiology 2005; 161: 526-535.
A Swedish Interphone Study reporting, "For regular mobile phone use [there was no risk] for glioma... and for meningioma."
[6] Christensen et al, (April 2005) Cellular telephones and risk for brain tumors: A population-based, incident case-control study, Neurology. 2005 Apr 12 ;64 (7): 1189-95. Erratum in: Neurology. 2005 Oct 25; 65 (8):1324
A Danish Interphone Study of glioma and meningioma reported, "The overall analyses did not reveal an increased risk for ... regular use of a cellular telephone ..."
[7] Schüz et al, (March 2006) Cellular Phones, Cordless Phones, and the Risks of Glioma and Meningioma (Interphone Study Group, Germany), American Journal of Epidemiology 2006 Mar 15; 163 (6): 512-20. Epub 2006 Jan 27.
A German Interphone Study reporting, "For regular cellular phone use [there was no risk] ... for glioma and ... for meningioma."
[8] Takebashi et al, (2006) Mobile phone use and acoustic neuroma risk in Japan, Occupational Environmental Medicine, 2006; 63; 802-807.
A Japanese Interphone Study reporting, "No significant increase of acoustic neuroma risk was observed ... when regular mobile phone ... was [used]."
[9] Klaeboe et al, (2007) Use of mobile phones in Norway and risk of intracranial tumours, European Journal of Cancer Prevention 2007, 16:158-164.
A Norwegian Interphone Study reporting, "No increased risk was observed for gliomas, meningiomas ... and acoustic neuromas ... among regular mobile phone users ..."
[10] Hours et al, (October 2007) Cell Phones and Risk of brain and acoustic nerve tumours: the French INTERPHONE case-control study, Revue d'Épidémiologie et de Santé Publique 2007 Oct, 55 (5): 321-32. Epub 2007 Sep 11. French.
A French Interphone Study reporting, "Regular cell phone use was not associated with an increased risk of neuroma ..."
[11] Hepworth et al, Mobile phone use and risk of glioma in adults: case-control study, BMJ Online First bmj.com.
A United Kingdom Interphone Study reporting, "Overall, we found no raised risk of glioma associated with regular mobile phone use ..."
[12] Sadetzki et al, (December 2007) Cellular Phone Use and Risk of Benign and Malignant Parotid Gland Tumors - A Nationwide Case-Control Study, American Journal of Epidemiology Advance Access published December 6, 2007.
An Israeli Interphone Study.
[13] Lönn et al, (October 2006) Mobile phone use and risk of parotid gland tumor, American Journal of Epidemiology 2006 Oct 1; 164 (7): 637-43. Epub 2006 Jul 3.
A Swedish Interphone Study.